
Good News About a Bad Kind of Stress
By Marcus Moore, MD and Douglas Mulhall
*This is an article from the Winter 2024 issue of Combat Stress
The American Heart Association (AHA) has declared low levels of heavy metals such as lead, cadmium, and arsenic to be major heart disease risks. These are found in drinking water, soil, consumer products, food, and smoke from wildfire and cigarettes, and also in emissions from weapons discharge and explosions, burn pits, and diesel engines. These hidden stressors accumulate over time in humans, causing chronic inflammation and other disease-triggering problems.
The AHA also identified a therapy that improves effectiveness and slashes the cost of treating peripheral artery disease plaguing 10 million Americans, including combat Veterans. The therapy can also reduce the damage from heavy metals ingested by military personnel in the line of duty.
Those metals provoke a different kind of stress than most people would realize. This is called oxidative stress, which causes chronic inflammation and tissue damage when it spirals out of control. Oxidative stress is also linked to mental health disruptions that increase emotional stress.1 Due to these links, it makes sense to examine how military personnel are exposed and what can be done to resolve and alleviate this.
Militaries frequently operate in remote and austere environments. These living conditions can range from temporary and fixed shelters to ships. The environments may lead to environmental exposures that are seldom experienced by the general population. Furthermore, training and combat-related tasks, including operating in armoured vehicles or training on weapon ranges, may expose military members to heavy metals.2,3
Service Members work for up to 6 months on ships, living in close quarters, including the machinery and weapons they manage. Many naval ships are powered by electricity generated with combinations of gas and diesel. Arsenic is a known product of diesel combustion, while onboard exposure to other heavy metals can come from welding,4 tire particles on aircraft,5 and weapons discharge.
Service Members are routinely exposed to lead from discharging or cleaning firearms.6 Military health services have worked to limit or track exposure, including periodic measurement of lead levels for certain trades, but once again, the overall risk cannot be eliminated.
While the Armed Forces has extensive environmental and occupational health programs,7 other studies have identified gaps in information gathering across operations,8 which make it difficult to determine the total heavy metals exposure experienced by military personnel.
A priority for the Armed Forces is maintaining a fit force. Services Members are subject to routine screening at more frequent intervals than the general population; however, routine screening for heavy metals is not included in all trades. This is despite the growing body of research behind the role heavy metal exposure plays in the development of cardiovascular disease.9 Furthermore, due to recruiting and retention issues, the military may be more inclined to retain members with cardiovascular disease risk factors that they may have released before. This means that military health services may have to explore treatments for both heavy metal exposure and cardiovascular disease that were previously not covered. 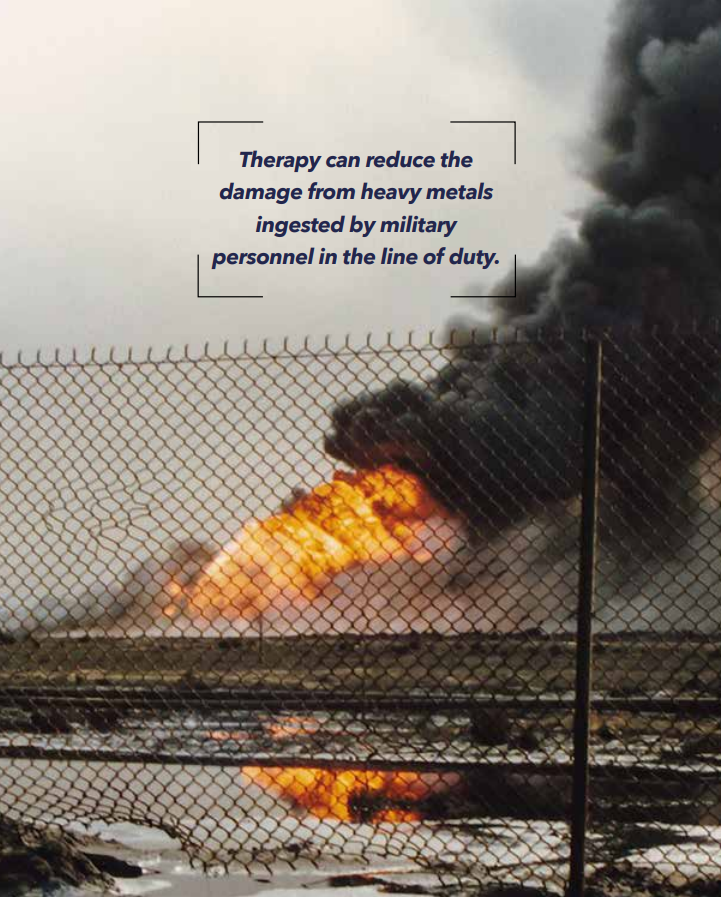
This is where a therapy identified by the AHA comes in. For years, the method known as chelation therapy had a checkered reputation due to apparent lack of clinical proof supporting its efficacy. During chelation, a heavy metal binder, such as EDTA (Ethylenediaminetetraacetic acid – a widely used food preservative also used to treat heavy metal poisoning), is injected intravenously. It chemically binds to, or “grabs” heavy metals, which are then excreted from the body. A $35 million clinical trial known as the Trial to Assess Chelation Therapy (TACT) proved, over a ten year period, that this therapy is not only safe when administered with multivitamins under medical supervision, but also reduced all causes of death in diabetic heart patients by 41 percent.10 This was further supported by a clinical study that prevented amputations in patients with Peripheral Artery Disease (PAD) that blocked arteries in their legs.11 In each case, patients excreted heavy metals, ranging from lead and cadmium, to gallium and tin. As the metals were excreted, the lesions on patients’ legs healed, and circulation to the affected limbs was restored, preventing amputation.
Regular blood and urine tests that are used in standard-of-care practiced by most providers did NOT reveal the extent of contamination prior to therapy, because the metals reside mostly in tissue, not in the blood. Hair and nail samples can give some indication, but a more reliable way is to use the protocol from the PAD studies, as those provide comparative data. In those studies, the standard-of-care tests were used as a baseline, then urine samples were periodically measured following IV therapy with EDTA. The differences between baseline and post-therapy were substantial.11
Another study compared chelation with standard medical practice for PAD and found that chelation cost 80 percent less than standard practice. The comparative study found that costs for this method cost $8,000 to $16,000, compared to $78,000 to $116,000 for standard care covered by most insurance schemes.12
Be forewarned that despite years of clinical studies, the method described in the AHA official statement is still labeled as unreliable and risky by healthcare authorities who are not familiar with the most recent results or are skeptical about them. The supervisor of the trials, Dr. Gervasio Lamas, Chief of Cardiology at Columbia University, indicated that he used to be one of those skeptics. He started the TACT trials to prove that chelation did not work. Much to his surprise, it did. Results were published in the highly ranked journal, Circulation.
In summary, the new AHA declaration that these heavy metals are heart disease risk factors, combined with results of clinical trials and studies, suggest that it is completely sensible to upgrade screening of military personnel returning from combat tours of duty, or who are regularly exposed to heavy metals such as lead, arsenic, and cadmium, and to consider therapy if low or greater levels of the metals are detected. The potential benefits are compelling: keep Service Members fit for duty longer, prevent later healthcare costs associated with heavy metals exposure, and give personnel the psychological confidence that while some exposures can’t be prevented, the damaging effects can.
References
- Ayuso-Álvarez, A., L. Simón, O. Nuñez, C. Rodríguez-Blázquez, I. Martín-Méndez, A. Bel-lán, G. López-Abente, et al. Association between heavy metals and metalloids in topsoil and mental health in the adult population of Spain. Environmental Research, 179, 2019. https://doi.org/https://doi.org/10.1016/j.envres.2019.108784.
- Environment, and Climate Change Canada. 2018. Lead Ammunition: Executive Summary. April 5, 2018. https://www.canada.ca/en/environment-climate-change/services/management-toxic-substances/list-canadian-environmental-protection-act/lead/using-more-lead-free-ammunition/lead-ammunition-executive-summary.html.
- Laidlaw, Mark A. S., Filippelli, Gabriel, Mielke, Howard, Gulson, Brian and Ball, Andrew S. Lead exposure at firing ranges-a review. Environmental Health: A Global Access Science Source, 16(1), 2017: 34.
- Su, Ting-Yao, et al. Effects of heavy metal exposure on shipyard welders: a cautionary note for 8-Hydroxy-2’-Deoxyguansoine. International Journal of Environmental Research and Public Health. 16.23, 2019: 4813.
- Vanessa, Spanheimer and Katrakova-Krüger, Danka. Analysis of tire wear airstrip particles (TWAP). Scientific Reports, 12:1, 2022: 15841.
- Nili, Greenberg, Frimer, Ron, Meyer, Robert, Derazne, Estella and Chodick, Gabrial. Lead exposure in military outdoor firing ranges. Military Medicine. 181 (9), 2016: 1121-26.
- Jeffrey, Drezner et al. Incorporating environmental considerations into defense acquisition practices. 2023. https://apps.dtic.mil/sti/trecms/pdf/AD1213388.pdf.
- L. Krahl, Pamela, Mirza, Raúl A. and Rice, William A. The capability gap in occupational health information management. Military Medicine, 187:11-12, 2022: 319-322, https://doi.org/10.1093/milmed/usac233.
- Rajiv, Chowdhury, Ramond, Anna, O’Keefe, Linda M., Shahzad, Sara, Kunutsor, Setor K., Muka, Taulant, Gregson, John, et al. Environmental toxic metal contaminants and risk of cardiovascular disease; systematic review and meta-analysis. British Medical Journal. 362, 2018: k3310.
- Lamas, Gervasio A., Boineau, Robin, Goertz, Christine, Mark, Daniel B., Rosenberg, Yves and Stylianou, Mario et al. EDTA Chelation therapy alone and in combination with oral high-dose multivitamins and minerals for coronary disease: the factorial group results of the trial to assess chelation therapy. American Heart Journal 168:1, 2014: 37-44. e5. https://doi.org/https://doi.org/10.1016/j.ahj.2014.02.012.
- Arenas, I., Ujueta, F., Diaz, D., Yates, T., Olivieri, B., Beasley, R. and Lamas, G. Limb Preservation using edetate disodium-based chelation in patients with diabetes and critical limb ischemia: an open-label pilot study. Cureus 11: 12, 2019: e6477. https://doi.org/10.7759/cureus.6477. https://www.ncbi.nlm.nih.gov/pubmed/32025401.
- Porudominsky, Ruben, Ujueta, Francisco, Arenas Ivan A., Lamas, Gervasio A. Preliminary cost estimates of edetate disodium infusions for critical limb ischemia in patients with diabetes mellitus. Vascular Disease Management. 17(7):2020; E137-E141.

{kind=link}